Innovation in Action: Eight Health Centers Target Financial Sustainability
NACHC Blog
NACHC’s Center for Innovation has launched the 2026 Innovation Incubator program. This year, the cohort focuses on the theme of Financial Diversification & Sustainability. In its third iteration, the Incubator operates on the premise that innovation often fails when “fixers” jump to solutions without understanding the root cause. To shift this dynamic, the program provides seed funding and a “sandbox” to test new ideas without immediate real-world consequences. NACHC’s Incubator training relies on collaborative growth, where health centers convene in person and during virtual meetings to learn and implement innovation concepts through NACHC’s reinvigorated Innovation Incubator Curriculum
The eight selected health centers receive funding, training, and access to subject matter experts over a 9-month period to design sustainable and replicable solutions. The 2026 cohort includes:
The cohort recently completed an intensive in-person training on March 26 and 27, 2026. On day one, participants engaged in “Brain Blasts” to generate a wide array of ideas and approaches to their specific patient-centered challenges.
“I like how we were pushed in uncomfortable directions. Even if we didn’t go all the way, we landed in an advanced place based on the push and compromise.” – Workshop Participant
“I loved all the touch points with other health centers. It really made the experience very helpful.” – Community Health Service, Inc.
On day two, the training transitioned from theoretical concepts to testable actions. Teams identified risky assumptions and used “scrappy” tools like storyboards and rudimentary drawings to prototype their ideas. In doing so, the health centers were able to devise plans to progress quickly and gather rapid feedback from staff and patients before investing significant resources.
“Being in the room with peers and SMEs allowed us to test, refine, and strengthen ideas in real time. Hearing how other health centers are approaching similar challenges was also helpful and expanded our thinking. A key takeaway for our team was grounding our Big Idea and prototypes in what we heard during staff, patient, and community interviews. The process helped us turn what we heard from our community into something real, testable, and sustainable.” – Waianae Coast Comprehensive Health Center
After the training, the health centers jump into testing multiple components of their idea on staff and patients. This summer, they’ll develop a business plan and prepare for a full pilot to ensure that their patient-centered solution is able to generate revenue for long-term sustainability. The 2026 program will culminate in a live pitch session in the fall, where health centers will show off their hard work to industry experts and stakeholders.
Click the link below if you’d like to stay connected by sharing your contact information with NACHC’s Center for Innovation!
Across the United States, Community Health Centers (CHCs) have become the primary delivery system for pediatric care, especially among the nation’s populations with limited access to health care. They serve nearly 10 million children annually, about 1 in every 7 in the country. This is not a peripheral role in the health system – it represents a central responsibility for delivering cost-effective primary care and preventive health services to children at high risk for complex health conditions.
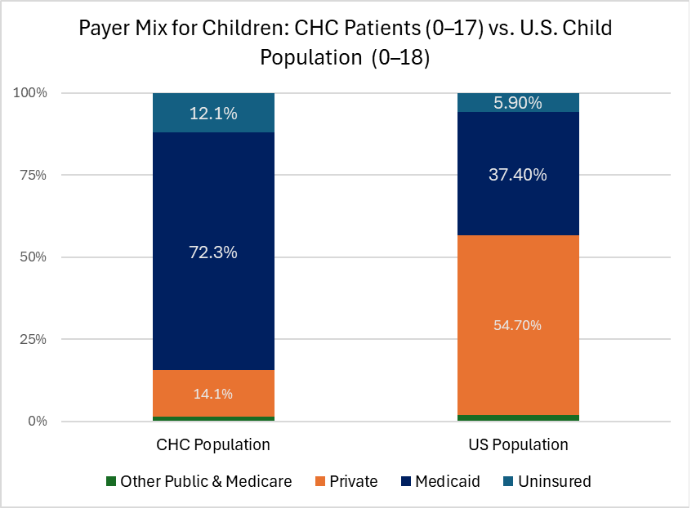
CHCs’ role becomes clearer when insurance coverage is considered. In 2024, more than 70% of children receiving care at CHCs relied on Medicaid, and another 12% were uninsured. This stands in sharp contrast to the overall CHC patient population, where about half depend on Medicaid and 18% lack insurance. Across the broader US child population, just 37% of children under 19 were covered by Medicaid in 2024, and only 6% were uninsured. Overall, CHCs provide care to roughly one in four Medicaid-covered and one in four uninsured children nationwide, focusing resources on those most at risk of care gaps.
Data Sources: Bureau of Primary Health Care. (2024). Uniform Data System. Health Resources and Services Administration, U.S. Department of Health and Human Services.
This is not incidental. Medicaid is now the dominant insurer for children, and CHCs have become its most important delivery platform. With significant Medicaid financing changes on the horizon, CHCs will face increased financial strain and administrative burden. The needs most directly affected include coverage continuity for children, payment stability for pediatric visits and developmental screenings, behavioral health integration, and care coordination. As coverage policies shift, CHCs will experience increased pressure as frontline providers for millions of families.
Children, Adolescents, and School-based Care
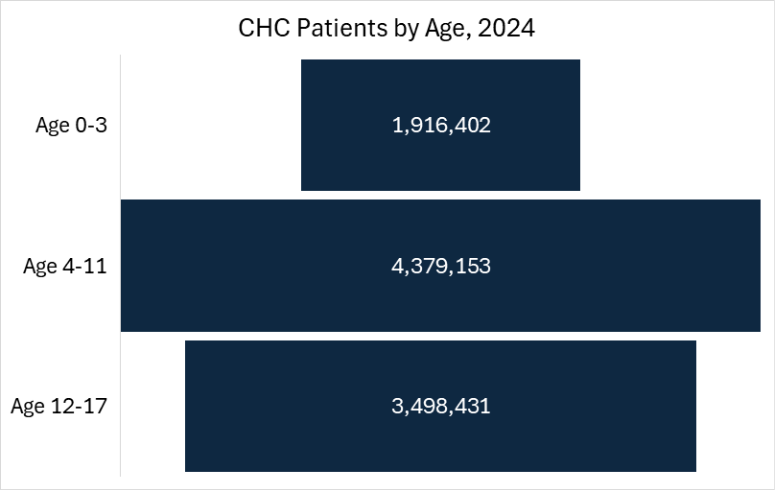
Children of all ages rely on CHCs, but some groups stand out. In 2024, nearly 4.4 million children seen at CHCs were ages 4-11, making them the largest pediatric age group served. These are the years when asthma, obesity, learning difficulties, and developmental delays are most often identified and addressed. Another 3.5 million adolescents received care at CHCs. Among adolescents, needs increasingly include behavioral health assessment, depression and anxiety screening, substance abuse screenings, and chronic disease management. Early identification and treatment during adolescence can substantially alter long-term health trajectories.
Data Source: Bureau of Primary Health Care. (2024). Uniform Data System. Health Resources and Services Administration, U.S. Department of Health and Human Services.
CHCs also operate more than 4,400 school‑based health centers (SBHC)—at least two‑thirds of all SBHCs nationwide—bringing care directly into the places where children spend much of their day. For Medicaid-covered and uninsured children, school-based sites are often the only reliable point of access to consistent care during the school year. These sites are especially important for families facing transportation barriers or limited access to pediatric specialists.
Taken together, these numbers show that CHCs are embedded in children’s everyday lives, managing chronic disease, identifying developmental needs, and supporting academic success through health.
The Workforce Behind Pediatric Care
To meet the needs of nearly 10 million young patients, CHCs rely on a comprehensive and dedicated workforce. In 2024, they employed more than:
3,400 pediatrician FTEs, who collectively provided over 10 million visits
7,600 family physicians, who delivered more than 19 million visits
Thousands of nurse practitioners, physician assistants, behavioral health clinicians, and other essential providers
This blended workforce reflects the reality that in high-need communities, pediatric care is delivered through integrated primary care teams that must address medical, behavioral, and social complexities simultaneously. Within this care model, CHCs conducted 2.6 million childhood development screenings and evaluations for 1.8 million young patients. These screenings are the front line of early intervention, identifying speech delays, behavioral disorders, and chronic conditions before they become permanent barriers to learning and health.
Every one of those screenings reduces downstream costs in special education, emergency care, and disability services. However, delivery is dependent on stable staffing, adequate service payments, and the infrastructure to coordinate follow-up care.
Preventive Care on the Rise
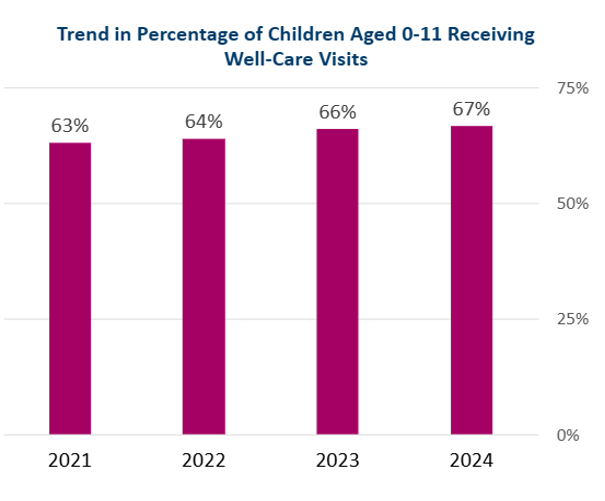
Preventive care remains one of the core strengths of CHCs. In 2024, 67% of children ages 0–11 received a well‑child visit at a CHC—a rate that has increased even as workforce shortages and financial pressures have intensified. These visits are the foundation of pediatric medicine, which includes growth and development monitoring, behavioral health screening, and anticipatory guidance that shapes health for decades.
Data Source: Bureau of Primary Health Care. (2021–2024). Uniform Data System. Health Resources and Services Administration, U.S. Department of Health and Human Services.
When preventive care is consistent, children are healthier, schools are stronger, and communities face fewer avoidable medical and social costs. For Medicaid-covered and uninsured children, CHCs are often the only place where this continuity exists.
A Strategic Imperative
CHCs now operate as the nation’s largest primary care system for low-income children. The data is unequivocal: 1 in 7 of the pediatric population depends on CHCs for routine care, developmental screening, behavioral health, and early intervention. That means Medicaid and CHC policy, in practice, is pediatric policy. Changes in eligibility, payments, workforce support, or federal grant funding directly impact children’s access to reliable care and healthier long-term outcomes.
This also creates a new opportunity. With millions of children receiving continuous, community-based care, CHCs represent the most scalable platform in the country for improving early-life health and controlling long-term costs through prevention. Policymakers should recognize CHCs as the primary delivery system for pediatric care. Aligning Medicaid, workforce, and federal funding with that reality should be the defining task for child health policy.
In 2024, seven million patients relied on Community Health Centers (CHCs) for routine, emergency, restorative, and rehabilitative dental services. With a workforce of over 5,700 full-time equivalent (FTE) dentists, 3,000 dental hygienists, and more than 13,000 additional dental professionals, CHCs delivered 16.8 million dental visits nationwide.
More than 80% of CHCs (1,227 of 1512 CHCs) provided dental care, making them a critical access point for millions of publicly insured Medicare and Medicaid enrollees and low-income patients. Despite this availability, approximately two in three patients still had unmet oral health needs, highlighting persistent challenges in coverage, workforce capacity, and access. Nationally, the gap in dental coverage remains substantial. According to the 2024 State of Oral Health Equity in America survey, 27% of U.S. adults (approximately 72 million people) lack dental insurance.
Preventive Care at the Core, but CHCs Also Address Complex Oral Health Needs
Preventive care forms the backbone of CHC dental care. Oral exams and cleanings (prophylaxis) accounted for 60% of all dental visits. These services are critical for early identification of oral disease and create opportunities to detect signs of systemic conditions. Restorative, rehabilitative, and emergency care address more complex or episodic needs, from fillings and crowns to root canals and oral surgery. While most patients receive routine preventive services, a smaller subgroup require more intensive interventions, emphasizing the balance CHCs must strike between preventive care and high-need, resource-intensive cases.
In 2024, dental sealant rates for children aged 6 to 9 reached about 60 percent in rural and urban CHCs, outperforming the national average of under 50 percent. This demonstrates consistent delivery of evidence-based preventive care across diverse communities, despite workforce and infrastructure challenges.
Source: 2024 UDS data (HRSA). Includes Look-alikes.
Delivering Care Under Workforce Pressures
CHC dental teams operate on a remarkable scale. On average, each dentist handles over 2,300 visits annually, or about 45 visits per week. Hygienists average an additional 1,100 visits. However, the CHC dental workforce is under considerable pressure, with 21% of dental hygienists and assistant positions vacant and turnover rates of 21% for dentists and 18% for dental hygienists and assistants. These gaps limit capacity to meet patient demand, illustrating both the efficiency of and strain on CHC dental teams.
Providing Care in a Fragmented System
In 2024, CHCs spent more than $5 billion delivering dental services, which translates to about $700 per patient. However, these costs were not fully reimbursed.
Medicaid: Comprehensive dental services are covered for children in every state, but adult dental benefits vary widely because they are classified as optional under federal Medicaid rules. Some states provide only emergency care; others limit the services or exclude adult dental services entirely.
Medicare: Routine dental services, including exams, cleanings, fillings, dentures, and most extractions, are not covered.
Private: Many plans impose annual benefit caps and restrict coverage for restorative and preventive services, functioning more like a discount program than comprehensive insurance.
Preventive dental care is also not considered an Essential Health Benefit for adults under federal law, which means states and insurers are not required to cover it.
Even when patients have dental insurance, access is far from guaranteed. Many dental providers do not accept Medicaid or Medicare due to low reimbursement rates, leaving CHCs as one of the few consistent access points for publicly insured or uninsured patients seeking dental care.
Making an Impact Beyond the Dental Chair
Oral health affects more than just teeth. Pain, infection, and untreated disease can reduce productivity, with Americans losing more than 243 million hours of productivity each year to oral health problems. Untreated dental disease is estimated to cost the U.S. $45 billion annually in lost productivity. Poor oral health can also influence social interaction and employability.
When patients cannot access routine care, they frequently turn to emergency departments (EDs). Between 2020 and 2022, there was an average of 1.94 million ED visits annually for tooth disorders, often resulting only in temporary relief. Redirecting care to CHCs could save the health care system $1.7 billion each year, while providing patients with definitive treatment.
Looking Ahead
Millions of Americans turn to CHCs each year for dental care, often as their primary or only source of services. Strengthening their role means expanding Medicaid and Medicare coverage, particularly for adults, investing in the dental workforce to reduce vacancies and turnovers, supporting sustained funding to allow CHCs to meet patient demand, and integrating medical-dental care to help catch chronic diseases early and to maximize the impact of every visit.
CHCs are essential to delivering dental care that scales, bridging gaps in a fragmented system, and improving oral health outcomes for millions of Americans. Expanding access to oral health services not only improves individual patient health but also enhances workforce productivity, reduces avoidable emergency care, and strengthens the broader health care system.
This blog series shares ongoing updates on the Rural Health Transformation Program and what it means for Community Health Centers. Stay tuned for future posts exploring a wide range of related topics and emerging issues.
On December 29, the Centers for Medicare & Medicaid Services (CMS) announced that all states will receive awards under the Rural Health Transformation Program (RHTP). The RHTP will provide states with $50 billion over five years to expand access to care in rural communities, strengthen the rural health workforce, modernize rural facilities and technology, and support innovative models that bring high-quality, dependable care closer to home.
For Community Health Centers (CHCs), the focus now turns to how states will deploy these funds, and how CHCs can position themselves to access and implement these investments.
State Awards and Funding Distributions
In 2026, states will receive first-year RHTP awards from CMS averaging $200 million, with awards ranging from $147 million (New Jersey) to $281 million (Texas). The RHTP funding will average $144 per rural resident over the 5 years of the program. When examining discretionary grant funding per 1,000 rural residents, the distribution varies widely—from $26,611 in Michigan to $662,755 in Alaska. States had up to 30 days to submit revised budgets reflecting their final award amounts, which must be approved by CMS.
States are now advancing procurement processes to distribute RHTP funds to eligible entities. Approaches vary and include:
Direct allocations by Governors or state agency directors
Issuance of Requests for Proposals (RFPs)
Legislative appropriations
In North Dakota, recently enacted legislation appropriated RHTP funds to the Department of Health and Human Services and designated the Bank of North Dakota as administrator of a rural health medical facility infrastructure loan program. This structure provides short-term gap financing to grant recipients and offers a model for states seeking to pair grants with financing tools.
Several states are also leveraging third-party entities to manage funding distribution and oversight. In Rhode Island, a Rural Stakeholder Advisory Committee was established to monitor changes in costs, quality, outcomes, and patient experience, and to guide reinvestment and sustainability strategies. The Committee designated the Rhode Island Health Center Association—the state’s Primary Care Association—to oversee funding allocations to CHCs participating in initiatives such as value-based payment transitions, technology modernization, and mobile health services.
Below (Table 1) is an overview of recent RHTP award announcements and funding opportunities across several states.
Looking Ahead: Positioning Community Health Centers for Success
The $50 billion investment from Congress presents a once-in-a-generation opportunity to reshape rural health care delivery. The choices states make in the months ahead—around procurement strategies, partnerships and performance expectations—will determine whether this funding drives lasting system transformation or short-term gains. For CHCs, this is a pivotal moment to engage early, align strategically and lead collectively.
As states move forward with multiple award pathways, health centers and PCAs should, where appropriate, present a unified and coordinated approach that clearly demonstrates the value of investing in community-based primary care. By showcasing how health center systems collaborate, leverage shared infrastructure, and deliver measurable impact, they can put forward strong, high-impact proposals that position primary care as the foundation of rural transformation. CMS and state leaders are encouraging interested parties to get prepared. This includes regularly checking your state’s RHTP websites for updates, assessing where health centers align with prospective projects, and identifying RFPs/funding opportunities that advance your state’s RHTP goals.
Table 1. Recent RHTP award announcements and funding opportunities across states
Gov. Kim Reynolds announced the nation’s first RHTP awards in January, totaling more than $78.6 million. Of that amount, $12.6 million was allocated through the state’s Health Care Workforce Recruitment initiative, which supports the recruitment of highly skilled providers by offering competitive incentives such as recruitment bonuses, relocation assistance, and other strategies designed to make rural practice attractive and sustainable. Among the awardees, the Community Health Centers of Southeastern Iowa received funding for its Des Moines County and Lee County locations to strengthen its pediatric workforce, including recruitment and development of pediatricians (MD/DO) and pediatric physician assistants.
Ohio’s Department of Health released its first three requests for proposals focused on pharmacy and workforce initiatives. The Pharmacy Initiative RFP will award an estimated $2 million to equip pharmacists with the tools and training needed to operate. The Rural Health Workforce Pipeline; Pathways Upskilling and Retention RFP will provide up to $10 million across two rounds. In partnership with academic and training institutions, projects will support career exploration, community health worker upskilling, education pathways, rural apprenticeships, recruitment and retention incentives, and six-month housing stipends for providers who commit to at least 5 years in rural communities.
Announced multiple RFPs, including an FQHC value-based care (VBC) transformation initiative that will support rural health care providers and FQHCs to move towards VBC, including preparing to take on upside and downside risk and accountability for total cost of care and population health outcomes ($24.322 million). Additional RFPs include competitive awards to support sustainable food-is-medicine initiatives ($1.648 million), start-up costs for the state’s first four-year medical school ($42.5 million), and more.
Announced applications for the $44 million Regional Partnership Grant Program (RPGP). The program supports collaborative arrangements among eligible providers to promote preventive care, address the root causes of disease, improve efficiency and sustainability for rural providers, strengthen the health care workforce, advance value-based care models, and encourage the adoption of innovative technologies. Applications are due April 3, 2026.
Released a Request for Applicants to establish North Carolina Rural Organizations Orchestrating Transformation for Sustainability (“NC ROOTS”) Hubs. These regional organizations will help advance efforts across primary care, behavioral health, workforce development, value-based payment, and digital health, tailoring strategies to the unique needs of their regions. The initiative includes $235,513,062 in total grant funding (approximately $40 million per region), distributed across up to six NC ROOTS Hub Leads.
Issued an RFP for a Chronic Disease Management Navigation and Education Initiative. Funded projects will expand community-based education, care navigation, and self-management support for individuals living with chronic conditions such as diabetes, cardiovascular disease, asthma, and other long-term health challenges.
Released its first round of RFPs, including Preventive Health Initiatives ($8 million), Technology Solutions, Telehealth, and Remote Patient Monitoring ($9 million), Training and Capacity Building ($500,000), and a Rural Health Clinical Workforce and Retention Incentive program ($10 million).
Announced their first round of RFPs, which includes investments to expand and strengthen the rural Community Health Worker workforce and to create a population-based alternative payment methodology for primary care.
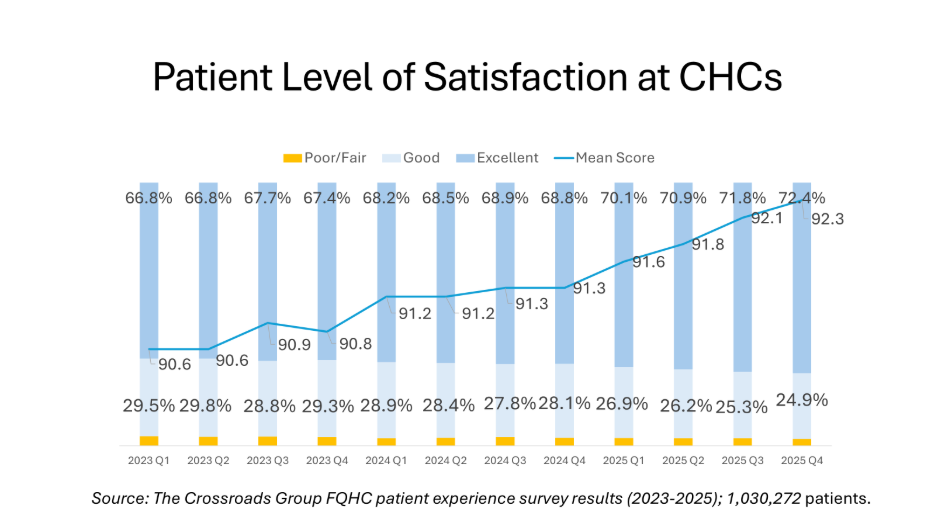
For another consecutive year, Community Health Centers (CHCs) across the country have maintained patient satisfaction rates above 90%, with national scores continuing to rise. In a health care environment where many patients describe growing frustration with access, continuity, and affordability, these results signal something important – CHCs are sustaining trust at scale among the 52 million patients they serve.
Patient experience survey data collected from 2023 through 2025 show over 72% of CHC patients selected the highest possible rating of Excellent, and more than 92% reported positive overall satisfaction. These findings reflect more than one million patient responses across diverse geographies, payer types, and community settings, making this one of the largest longitudinal patient experience datasets in primary care.
This remarkable consistency reflects more than good service. It reflects a care model that works, designed around patients rather than transactions. CHCs are community-governed providers that integrate medical, dental, behavioral health, and enabling services under one roof. Over time, those attributes translate into stronger engagement, more reliable access, and better management of chronic conditions.
The recent increase in CHC federal funding for FY 2026 provides important short-term stability for CHCs, helping CHCs maintain access, support their workforce, and respond to rising demand. Alongside federal investments, Medicaid coverage and payment policies will shape how CHCs deliver high quality care and maintain high levels of patient satisfaction.
These results offer important lessons for the broader health system. Integrated, team-based primary care models grounded in community governance consistently deliver a positive patient experience at scale. This success extends across a national network of over 1500 CHCs, serving tens of millions of patients each year in 17,000 communities.
For policymakers, the value proposition is clear. CHCs care for one in 10 people in the US annually and approximately one in four Medicaid enrollees annually, while accounting for less than three percent of Medicaid spending. High patient satisfaction rates reinforce that this model delivers quality and value, even while serving populations with high clinical and social complexity.
At the patient level, these results reflect more than favorable survey responses. High satisfaction indicates patients feel heard, respected and supported. This trust strengthens long-term relationships between patients and care teams and reinforces the role of CHCs as stable anchors in the communities.
CHCs are not simply maintaining patient satisfaction. They are sustaining it at a level many health systems aspire to achieve. Continued attention to the full federal and state policy landscape is critical to ensuring CHC patient access to quality care that communities value.
Community Health Centers (CHCs) are community-governed primary care clinics that provide high-quality primary care to all patients, regardless of ability to pay. They serve federally designated areas or populations and provide comprehensive services including primary care, dental care, vision services, mental health and substance use disorder services, and care coordination.
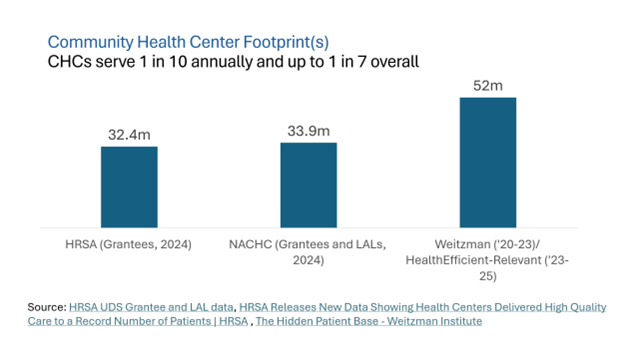
CHCs reach far more people than annual federal reporting alone suggests. Based on new data analysis from HealthEfficient, a health center-controlled network (HCCN) supporting approximately 60 CHCs, about 52 million people are connected to CHCs over time. This means up to one in seven people rely on CHCs for their primary care, up from one in 10 served based on single year reporting.
This finding aligns with prior estimates from the Weitzman Institute, which also estimated that up to 52 million unique patients received care from CHCs over a three-year period (2020-2023). Together, these independent analyses show that annual reporting substantially understates the full population served.
Annual Federal Reporting Captures Only One Year of Care
Official federal data show that CHC served 32.4 million patients in 2024. The National Association of Community Health Centers (NACHC) reports nearly 34 million patients served because it includes 153 look-alike health centers (LALs) alongside the 1,359 CHC federal grantees. Look-alike health centers meet all federal CHC grant requirements but do not receive federal CHC funding.
These annual counts reflect patients seen during a single year, but primary care relationships often extend beyond one reporting period. Many patients receive care intermittently, return after gaps, or cycle between coverage types such as Medicaid, commercial coverage, or period without insurance. Annual counts capture only part of the population that relies on CHCs over time.
CHC Network Data Confirm Greater Reach of CHCs
HealthEfficient, through aggregation by Relevant, analyzed patient populations across multiple years using shared data from participating CHCs. Their analysis found that the total number of unique patients connected to CHCs between 2023-2025 is approximately 1.5 times larger than the number seen in a single year, mirroring estimates from the Weitzman Institute. Applying this relationship to the 34.9 million patients reported annually results in an estimated reach of approximately 52 million people. This captures the full scope of CHCs’ role in providing comprehensive primary care across changing life circumstances, insurance transitions, and periods of increased need.
The following figure illustrates the difference between annual federal reporting of only CHC grantees, NACHC reporting that includes look-alikes health centers, and multi-year estimates from the Weitzman Institute and HealthEfficient-Relevant. It shows how annual counts reflect only part of the population connected to CHCs over time.
CHCs are a National Primary Care Foundation
Annual federal reporting remains essential for tracking year-to-year service delivery. Longitudinal analysis provides a clearer understanding of a broader population whose care depends on CHCs. Together, these perspectives show that CHCs serve not just tens of millions each year, but approximately 52 million people over time. CHCs are a foundational part of the US health care system, providing critical primary care to those at the highest risk of poor health outcomes.